
Quick Answer
Keratoconus cannot be reversed, but it can be stabilised and vision can be significantly improved. Treatment depends on severity and may include corneal cross-linking, specialist contact lenses, implantable contact lenses (ICL), or, in advanced cases, corneal procedures. Standard laser eye surgery is usually not suitable.
Understanding Keratoconus in Real Terms
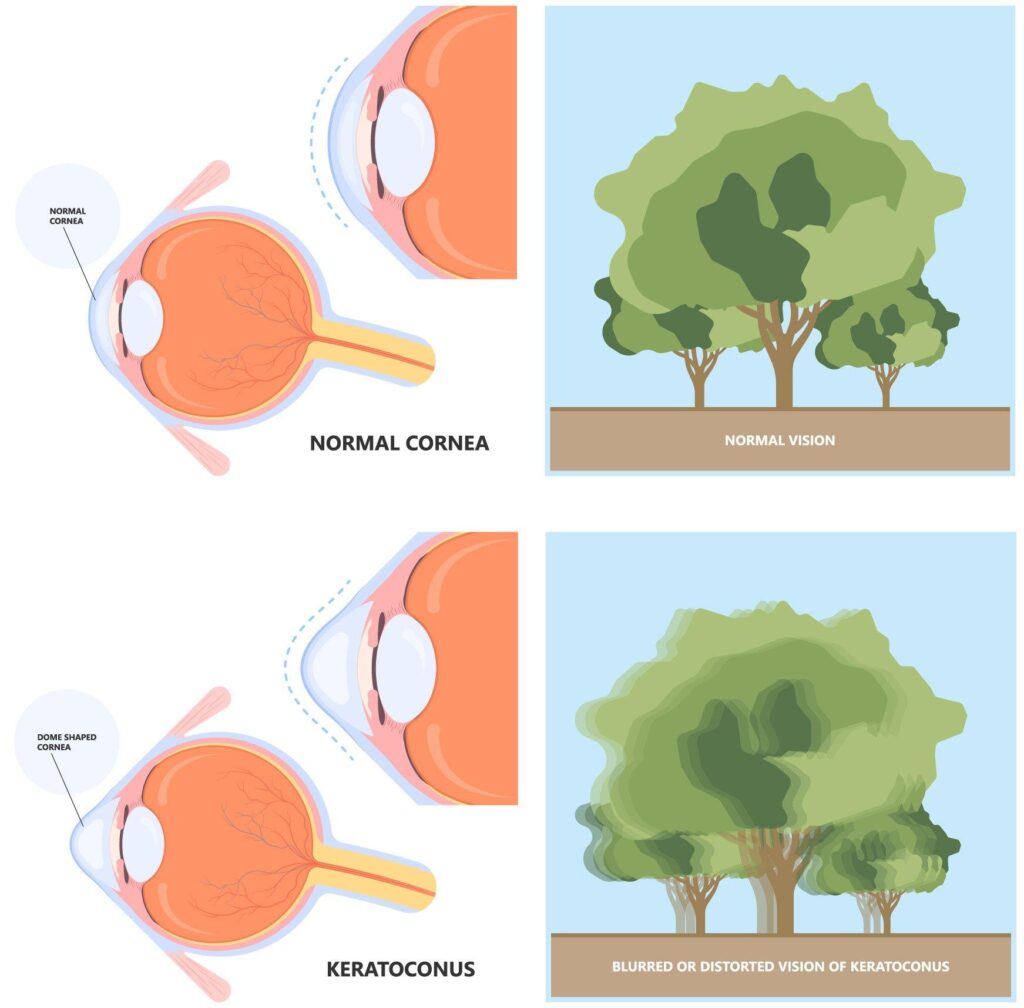
Keratoconus is not just a “blurry vision” problem.
It’s a structural change in the cornea, where the normally round surface becomes thinner and begins to bulge forward into a cone shape. That change affects how light enters the eye, which is why vision becomes distorted, not just out of focus.
Patients often describe:
- ghosting or double vision
- light streaking at night
- constant changes in prescription
Key point: this is not a simple refractive error, it’s a change in the shape of the eye itself.
Can You Have Laser Eye Surgery with Keratoconus?
In most cases, no.
Laser eye surgery works by reshaping the cornea. With keratoconus, the cornea is already weakened and irregular. Removing tissue can make the condition worse.
There are rare, highly selected cases where surface-based treatments may be considered alongside stabilisation, but as a general rule: standard LASIK or SMILE is not recommended for keratoconus.
How Do You Stop Keratoconus Getting Worse?
The first priority is stability.
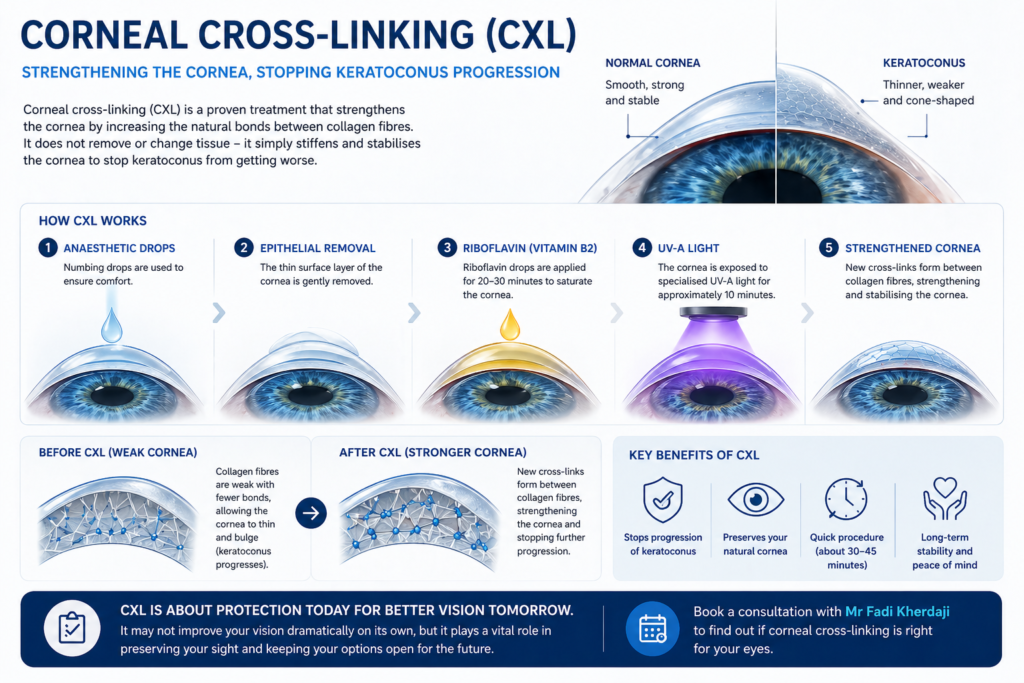
That’s where corneal cross-linking (CXL) comes in.
This treatment strengthens the cornea by increasing the bonds between collagen fibres. It doesn’t improve vision dramatically on its own, but it can stop the condition from progressing.
From a clinical perspective, this is often the most important step, especially in younger patients.
Can Vision Be Improved After Keratoconus?
Yes, and this is where treatment becomes more tailored.
1. Specialised Contact Lenses
Often the first step after stabilisation.
- Rigid or scleral lenses create a smooth optical surface
- They can significantly improve clarity
- However, they still require daily wear and maintenance
2. Implantable Contact Lenses (ICL)
In carefully selected patients, ICL can play a role.
This is not about fixing the cornea itself, but improving how light is focused inside the eye.
ICL may be considered when:
- keratoconus is stable
- the cornea is no longer changing
- there is a consistent prescription
The benefit here is quality of vision, particularly when glasses or soft lenses are no longer effective.
3. Intracorneal Ring Segments (ICRS)
These are small implants placed within the cornea to help reshape it.
They can:
- reduce irregularity
- improve lens tolerance
- make vision more manageable
They are often used as part of a staged approach.
4. Lens-Based Solutions (When Appropriate)
In some patients, particularly as the eye ages, lens-based correction may become part of the overall plan.
This is less about keratoconus itself and more about:
- improving overall optical quality
- reducing dependence on external correction
What About Severe Keratoconus?
In advanced cases, where the cornea becomes too thin or irregular:
corneal transplant procedures may be required
This is less common today thanks to early detection and cross-linking, but it remains an important option when needed.
So… What Is the Best Treatment?
There isn’t a single answer.
The pathway usually looks like this:
- Stabilise the cornea (cross-linking)
- Improve vision (lenses or optical correction)
- Refine vision (ICL or surgical options where appropriate)
Each stage builds on the last.
A Clinical Perspective from Practice
Most patients don’t come in knowing they have keratoconus.
They come in because:
- their glasses aren’t working anymore
- their prescription keeps changing
- night vision feels increasingly difficult
Once we map the cornea properly, the picture becomes clear.
From there, the goal is not just to improve vision today, but to protect it long term. That often means thinking in stages, stabilisation first, then refinement.
Keratoconus changes how we approach vision correction
It moves the conversation away from simple laser treatments and towards a more structured, personalised plan.
For some patients, that means stabilising early and maintaining good vision with lenses.
For others, it opens the door to advanced solutions like ICL once the eye is stable.
The important thing is timing, understanding where your eyes are now, and choosing the right step at the right moment.